
The Regrets of Committing Abortion.
Case Report. An 18-year-old gravida I para 0 female presented from an outlying facility I week after voluntary termination of 18 weeks gestation with complaints of severe abdominal pain, nausea, and vomiting. Exploratory laparatomy for presumed bowel obstruction revealed uterine perforation and bowel devitalization and necrosis, which required small bowel resection.
Induced abortion. This is an abortion that is brought about intentionally. It is also called artificial or voluntary termination of pregnancy. This is opposed to a spontaneous abortion (a miscarriage).
Abortion risks. Approximately 10% of women undergoing induced abortion suffer from immediate complications, of which one-fifth (2%) were considered major. However the majority of complications take time to develop and will not be apparent for days, months or even years. Major risks and complications of abortion are described below.
DEATH. Deaths occurs most following abortion than miscarriage, birth or no pregnancy. Women who had abortions were 3.4 times more likely to commit suicide compared to women who had not been pregnant in the previous year and 6 times more likely to commit suicide than women who delivered.
IMMEDIATE COMPLICATIONS. Approximately 10% of women undergoing elective abortion will suffer immediate complications, of which approximately one-fifth (2%) are considered life threatening. The nine most common major complications which can occur at the time of an abortion are: Infection, excessive bleeding, embolism, ripping or perforation of the uterus, anesthesia complications, convulsions, hemorrhage, cervical injury, and endotoxic shock. The most common “minor” complications include: Infection, bleeding, fever, chronic abdominal pain, vomiting, gastro-intestinal disturbances, and Rh sensitization. Although less common, serious injuries have also resulted from the perforation of the intestine or other organs by an instrument used in abortions.
Others are: Hematrometra (a collection or retention of blood in the uterine cavity), bowel and bladder injury, retained products of conception, failed abortion and undiagnosed ectopic pregnancies.
The risk of death following abortion remains higher in each of the first ten years following the abortion. The risk of death increases with each abortion, 45% after one abortion, 114% after two abortions, and 192 percent after three or more abortions.
CERVICAL, OVARIAN, AND LIVER CANCER: Women with a history of one abortion face a 2.3 times higher risk of having cervical cancer, compared to women with no history of abortion. Similar elevated risks of subsequent ovarian and liver cancer have also been linked to single and multiple abortions. These increased cancer rates for post-aborted women may be linked to the unnatural disruption of the hormonal changes which accompany pregnancy and untreated cervical damage or to increased stress and the negative impact of stress on the immune system.
UTERINE PERFORATION. Between 2 and 3% of all abortion patients may suffer perforation of their uterus, yet most of these injuries will remain undiagnosed and untreated unless laparoscopic visualization is performed. The risk of uterine perforation is increased for women who have previously given birth and for those who receive general anesthesia at the time of the abortion. Uterine damage may result in complications in later pregnancies and may eventually evolve into problems which require a hysterectomy.
CERVICAL LACERATIONS. Significant cervical lacerations occur in at least one percent of first trimester abortions. Latent post-abortion cervical damage may result in subsequent cervical incompetence, premature delivery, and complications of labor. The risk of cervical damage is greater for teenagers and for second trimester abortions.
PLACENTA PREVIA. Abortion increases the risk of placenta previa in later pregnancies (a life threatening condition for both the mother and her wanted pregnancy) by seven to fifteen fold. Abnormal development of the placenta due to uterine damage increases the risk of fetal malformation, perinatal death, and excessive bleeding during labor.
SUBSEQUENT PRE-TERM DELIVERIES AND OTHER COMPLICATIONS OF LABOR. Women who had one, two, or more previous induced abortions are, respectively, 1.89, 2.66, or 2.03 times more likely to have a subsequent pre-term delivery, compared to women who carry to term. Prior induced abortion not only increased the risk of premature delivery, it also increased the risk of delayed delivery. Women who had one, two, or more induced abortions are, respectively, 1.89, 2.61, and 2.23 times more likely to have a post-term delivery (over 42 weeks). Pre-term delivery increases the risk of neonatal death and handicaps. PRETERM BIRTH/HANDICAPPED NEWBORNS IN LATER PREGNANCIES. Abortion is associated with cervical and uterine damage which may increase the risk of premature delivery, complications of labor and abnormal development of the placenta in later pregnancies. These reproductive complications are the leading causes of handicaps among newborns. Prior induced abortions significantly elevate the risk of having a premature birth in the future.
ECTOPIC PREGNANCY. Abortion is significantly related to an increased risk of subsequent ectopic pregnancies. Ectopic pregnancies, in turn, are life threatening and may result in reduced fertility.
PELVIC INFLAMMATORY DISEASE (PID). This is a potentially life threatening disease which can lead to an increased risk of ectopic pregnancy and reduced fertility. Of patients who have a chlamydia infection at the time of the abortion, 23% will develop PID within 4 weeks. 20 to 27% of patients seeking abortion have a chlamydia infection. Approximately 5% of patients who are not infected by chlamydia develop PID within 4 weeks after a first trimester abortion.
ENDOMETRITIS. This is a post-abortion risk for all women, but especially for teenagers, who are 2.5 times more likely than women 20-29 to acquire endometritis following abortion.
INCREASED RISKS FOR WOMEN SEEKING MULTIPLE ABORTIONS. Women who have multiple abortions face a much greater risk of experiencing these complications. This point is especially noteworthy since approximately 45% of all abortions are for repeat aborters.
LOWER GENERAL HEALTH. Pregnancy loss, and particularly losses due to induced abortion, is significantly associated with an overall lower health. Multiple abortions correlated to an even lower evaluation of “present health.” While miscarriage was detrimental to health, abortion was found to have a greater correlation to poor health. These findings support previous research which reported that during the year following an abortion women visited their family doctors 80% more for all reasons and 180% more for psychosocial reasons.
INCREASED RISK FOR CONTRIBUTING HEALTH RISK FACTORS. Abortion is significantly linked to behavioral changes such as promiscuity, smoking, drug abuse, and eating disorders which all contribute to increased risks of health problems. For example, promiscuity and abortion are each linked to increased rates of PID and ectopic pregnancies. Which contributes most is unclear, but apportionment may be irrelevant if the promiscuity is itself a reaction to post- abortion trauma or loss of self-esteem.
INCREASED RISKS FOR TEENAGERS. Teenagers, who account for about 30 percent of all abortions, are also at much high risk of suffering many abortion related complications. This is true of both immediate complications, and of long-term reproductive damage.
PSYCHOLOGICAL COMPLICATIONS. Women who have had abortions are four times more likely to die in the next year than those who complete their pregnancies. This is a result of both psychological effects, which result in an increase of suicides and risk-taking behaviour, and an increase in deaths from other medical causes.
In a study of post-abortion patients only 8 weeks after their abortion, researchers found that 44% complained of nervous disorders, 36% had experienced sleep disturbances, 31% had regrets about their decision. There are significantly greater use of medical and psychiatric services among aborted women. Most significant was the finding that 25% of aborted women made visits to psychiatrists as compared to 3% of the control group. Women who have had abortions are significantly more likely than others to subsequently require admission to a psychiatric hospital. At especially high risk are teenagers, separated or divorced women, and women with a history of more than one abortion. Abortion is significantly linked with a two-fold increased risk of alcohol abuse among women.
SEXUAL DYSFUNCTION. According to research, 30% to 50% of women report experiencing sexual dysfunctions, of both short and long duration, beginning immediately after their abortions. These problems may include one or more of the following: Loss of pleasure from intercourse, increased pain, an aversion to sex and development of a promiscuous life-style.
Conclusion: Morbid, even potentially fatal, complications can occur as a result of pregnancy termination. The chronicle of abortion risks is enough to give the perpetrator regrets to last a life time. It is obvious that saying no to abortion is a wise choice.
“Abortion is Four Times Deadlier than Childbirth.”
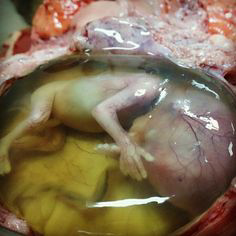
You were once like this in your mother’s womb. Some, sadly were aborted with aftermath chronicle of regrets by the perpetrators. BE PRO-LIFE.
.

Leave a Comment